This is the question no one asks at the prescribing appointment and everyone asks at 2 a.m.: What happens when I stop?
Not if — because most women stop eventually, whether because of insurance, cost, side effects, pregnancy plans, or the simple desire to not inject themselves every week for the rest of their lives. The real question is whether the body you’re working so hard to inhabit is rented or bought. Let’s look at what the actual research says, not the headlines.
The number you’re going to see everywhere
The most-cited study on this is the STEP 1 trial extension, published in Diabetes, Obesity and Metabolism in 2022. Participants who’d lost an average of 17.3% of their body weight over 68 weeks of semaglutide regained an average of 11.6 percentage points in the year after stopping.1 That’s about two-thirds of the original loss, regained in 12 months. A woman who had lost 40 pounds regained roughly 26 of them.

The cardiometabolic improvements — blood pressure, triglycerides, blood sugar — also largely reverted toward baseline.2 The benefits, in other words, weren’t permanent either.
Later trials have been more dramatic. STEP 10 showed more than 40% of lost weight regained within just 28 weeks of stopping. SURMOUNT-4 (the tirzepatide trial) showed more than 50% rebound over 52 weeks.3 A 2025 meta-analysis in eClinicalMedicine pooled 18 randomized trials and found an average weight regain of 5.63 kg (about 12 pounds) across the literature.4
This is the part most articles stop at, and it’s why the “ozempic face” headlines read the way they do. But if that’s the whole picture, it’s a misleadingly flat one.
The real-world distribution is more interesting
Clinical trial averages hide enormous individual variation. A 2024 analysis of real-world electronic health records from Epic’s Cosmos database tracked more than 20,000 semaglutide patients after they stopped the medication. The findings were genuinely nuanced:5
About 17.7% regained all the weight they’d lost or more. This is the “worst case” group.
But 55.7% either held their stopping weight or continued to lose. More than half.
In other words, a little over one in six women will regain everything. Well over half will keep most of what they earned. And there’s a broad middle range in between. You are not doomed to the average; you are somewhere on the distribution.
What determines which group you land in? That’s where it gets interesting.
Why the rebound happens biologically
Your body does not want to lose weight. This is not a lack of discipline; it’s a survival mechanism burned into 200,000 years of evolutionary history. When you lose weight — by any method, not just GLP-1s — several compensatory changes kick in and persist for years:

Hunger hormones rebound. Ghrelin (which drives hunger) goes up. Leptin (which signals fullness) goes down. Both can remain altered for years after weight loss.
Metabolic rate drops more than expected. A 150-pound woman who used to weigh 190 burns measurably fewer calories at rest than a woman who has always been 150. Your maintenance is not what a “normal” 150-pound body’s is.
Food noise returns. The intrusive food thoughts GLP-1s quiet come back. For some women, this is the most distressing part — more than the weight regain itself.
Fat cells remember. Research suggests that fat cells retain “metabolic memory” of being larger and preferentially refill when calories return.
This is why the newest research is reframing obesity as a chronic condition rather than a curable one — more like hypertension than like a broken arm. You wouldn’t stop your blood pressure medication once your blood pressure was normal. The medicine was what made it normal.
The flip side: if you stay on, the loss stays
The STEP 5 trial followed semaglutide users for 104 weeks of continuous treatment. Average weight loss at 52 weeks was −15.6%. At 104 weeks, it was −15.2%. Virtually identical. Minimal regain as long as the medication continued.6 This is the most important counterpoint to the “you’ll gain it all back” narrative: you mostly won’t, if you don’t stop.
The question is whether staying on indefinitely is desirable, affordable, or the right plan for you. Which brings us to what the research suggests helps you keep weight off if you do stop.
What actually predicts keeping it off
There’s no single large randomized trial answering this yet, but a consistent pattern emerges across the literature and clinical observation.
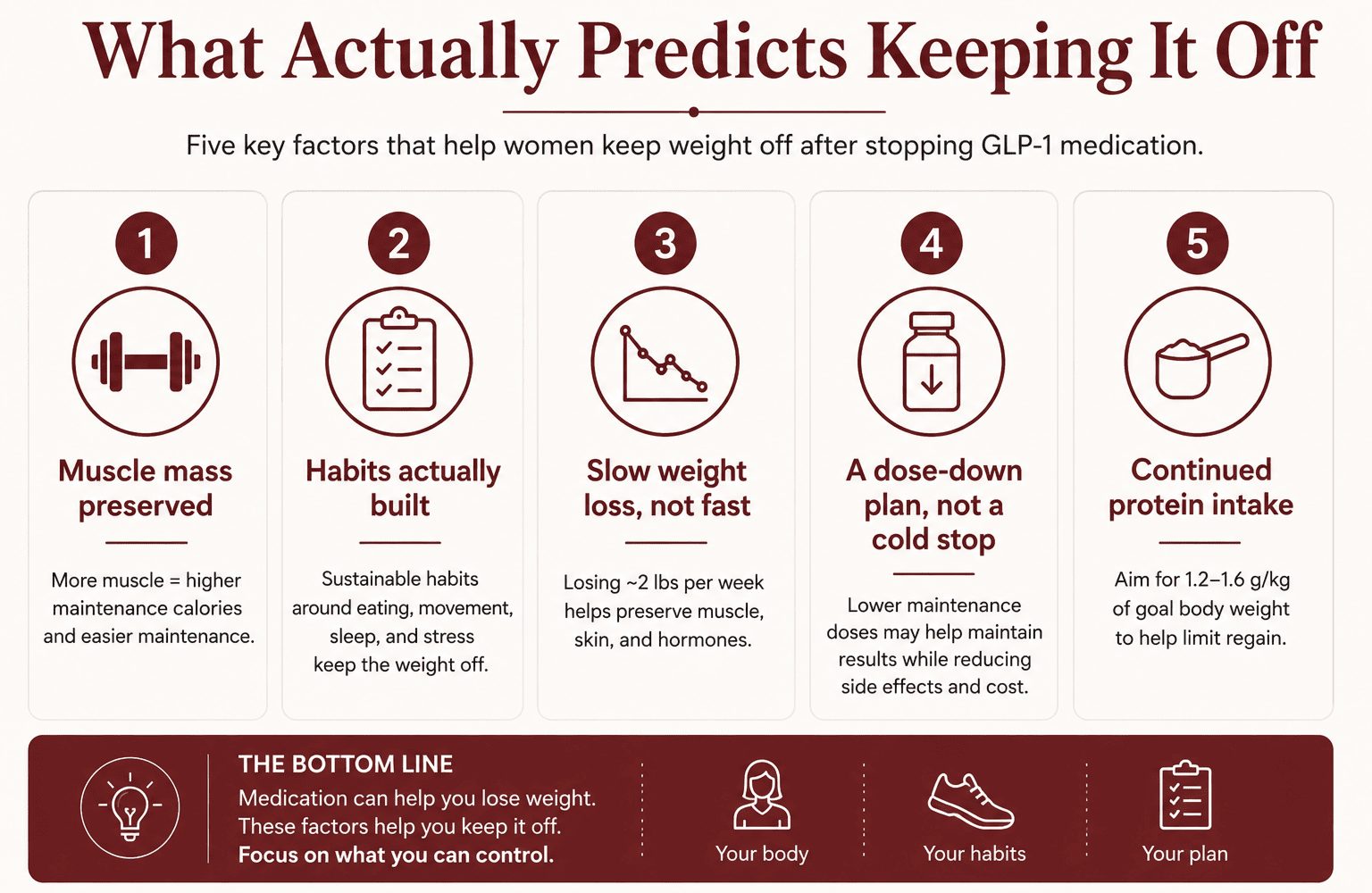
1. Muscle mass preserved. This is the biggest lever you control. If you lost 25 pounds of fat and 15 pounds of muscle on the way down, your maintenance calories are substantially lower coming off than they would have been. The less muscle you lost, the easier maintenance is. This is why protein intake and strength training on the way down aren’t “nice to have” — they are the infrastructure for life after the medication.
2. Habits actually built. Women who used the GLP-1 as cover to genuinely rewire eating patterns, exercise routines, sleep, and stress management tend to hold their loss. Women who used it as a magic wand tend not to. The medication can’t build habits for you, but it can give you months of reduced appetite during which habits are unusually easy to construct.
3. Slow weight loss, not fast. The STEP 1 data showed that participants with the fastest weight loss had the largest absolute regains. Losing 2 pounds a week preserves more muscle, more skin elasticity, and more hormonal equilibrium than losing 4.
4. A dose-down plan, not a cold stop. Increasingly, clinicians are using lower maintenance doses — rather than stopping abruptly — to help keep weight stable while reducing cost and side effects. This is a conversation to have with a prescriber, not a decision to make unilaterally.
5. Continued protein intake, in particular. A high-protein diet during and after maintenance (1.2–1.6 g/kg of goal body weight) is one of the only interventions with good evidence for limiting regain. If you’ve been using a nutrition shake specifically designed for GLP-1 users to hit those numbers, there’s no reason to stop using it just because the medication does — it’s a maintenance tool, not a pharmacology tool.
The bottom line
If you stop a GLP-1 and change nothing, the averages say you will regain about two-thirds of your weight loss within a year. If you use the time on the medication to build real muscle, real habits, and a real protein base, you can land in the majority of women who keep most of what they earned. If you stay on — even at a lower maintenance dose — the loss largely stays with you.
The story isn’t “it will all come back.” The story is: the medication buys you a window. What you build inside that window decides the rest.
This article is for informational and educational purposes only and is not medical advice. Decisions about starting, stopping, or continuing any medication should be made with your healthcare provider.
Sources
Wilding J.P.H. et al., “Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension,” Diabetes, Obesity and Metabolism, 2022. https://dom-pubs.onlinelibrary.wiley.com/doi/10.1111/dom.14725
STEP 1 extension — cardiometabolic reversion toward baseline (PMC). https://pmc.ncbi.nlm.nih.gov/articles/PMC9542252/
“Weight Regain After Liraglutide, Semaglutide or Tirzepatide Interruption: A Narrative Review of Randomized Studies,” MDPI, 2025. https://www.mdpi.com/2077-0383/14/11/3791
“Metabolic rebound after GLP-1 receptor agonist discontinuation: a systematic review and meta-analysis,” eClinicalMedicine, November 2025. https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(25)00614-5/fulltext
Epic Research / Cosmos, “Many Patients Maintain Weight Loss a Year After Stopping Semaglutide and Liraglutide,” 2024 — real-world database of 20,000+ patients. https://www.epicresearch.org/articles/many-patients-maintain-weight-loss-a-year-after-stopping-semaglutide-and-liraglutide
“Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial,” Nature Medicine, 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9556320/